20/20 vision with mild cystic macular changes; possible occult RVO versus VMT-related change reviewed.
Case Study: Mild Cystic Macular Changes with Good Vision
An optometrist uploaded this case to Care1.
A 77 yo female presented for a diabetic dilated fundus examination. The optometrist noted possible mild intraretinal fluid at the macula in the right eye and requested retina input regarding diagnosis and monitoring recommendations.
Best corrected visual acuity measured 20/20 OU. Intraocular pressure was 12 mmHg OD and 14 mmHg OS measured with non-contact tonometry. Anterior segment findings were unremarkable in both eyes.
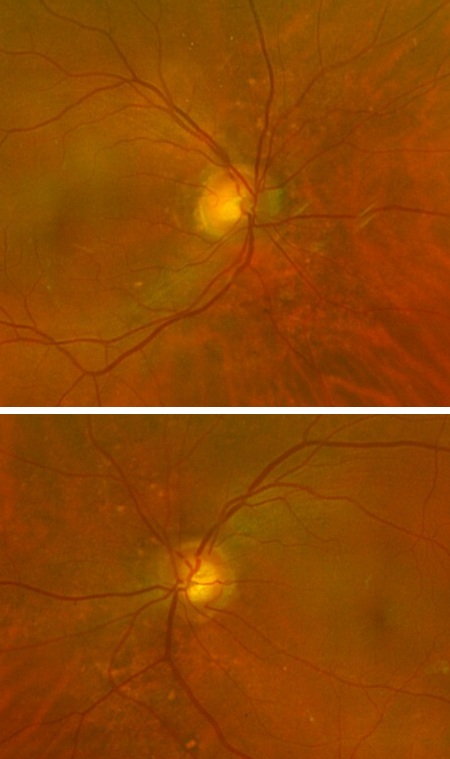
Posterior segment examination revealed clear lenses and vitreous OU. Optic nerves had healthy color and clear margins. Retinal vasculature demonstrated questionable mild venous dilation and tortuosity in the right eye, more apparent on OCT en face imaging than on widefield photography. The macula OD demonstrated mild focal cystic changes consistent with cystoid macular edema. The left macula appeared normal. There were no signs of neovascularization or retinal ischemia.
Given the patient’s preserved visual acuity and absence of neovascular or ischemic findings, would observation be appropriate, or should additional imaging or intervention be considered?
A retina specialist provided a virtual consult within 1-2 weeks through Care1. Scroll below to see their diagnosis.
Care1 Subspecialist’s Key Takeaways
This presentation is most consistent with mild cystoid macular edema in the right eye. There is subtle venous dilation and tortuosity that raises suspicion for an occult or remote retinal vein occlusion. The patient maintains excellent visual acuity and there are no signs of retinal ischemia or neovascularization.
Given the good vision and mild degree of edema, intravitreal treatment is not recommended at this time. Fluorescein angiography could help confirm the presence of vascular leakage but would be unlikely to change immediate management.
Systemic risk factor optimization is important. The patient should ensure regular follow-up with a primary care provider for blood pressure monitoring and routine laboratory testing, including screening for diabetes and dyslipidemia.
An in-person ophthalmology referral has been initiated. The optometrist can review this recommendation with the patient and coordinate through Care1 if they agree.
Care1 AI’s Clinical Insight
Cystoid macular edema represents the accumulation of extracellular fluid within the retinal layers, often forming round or petaloid cystic spaces on OCT. Retinal vein occlusion is a common vascular cause and may present subtly in mild or remote cases. Even in the presence of preserved visual acuity, careful monitoring is warranted, as progression can occur depending on vascular stability and systemic risk factors.
Did You Know?
Macular edema is the leading cause of vision loss in retinal vein occlusion and may occur even when retinal nonperfusion is minimal or not clinically obvious on examination.
Hayreh SS. Ocular vascular occlusive disorders: natural history of visual outcome. Prog Retin Eye Res. 2014;41:1–25.
Key Clinical Takeaway
A 77-year-old diabetic female presented with 20/20 vision OU and mild focal cystic changes consistent with cystoid macular edema in the right eye, detected on OCT despite minimal clinical symptoms.
Subtle venous dilation and tortuosity were noted OD without neovascularization or ischemia, prompting retina consultation for guidance on diagnosis and monitoring.
Would observation be appropriate, or should additional imaging or intervention be considered?