20/20–20/25 vision with ERM OD and lamellar macular hole OS; observation versus surgery reviewed.
Case Study: Stable Vision with Lamellar Hole
An optometrist uploaded this case to Care1.
A 63 yo male patient presented for a routine dilated fundus examination. The primary concern was previously documented epiretinal membrane in the right eye and a lamellar macular hole in the left eye. The optometrist noted that the findings appeared stable compared to prior visits and recommended annual monitoring but sought ophthalmology input.
Best corrected visual acuity measured 20/20 OD and 20/25 OS. Intraocular pressure was 23 mmHg OD and 20 mmHg OS measured with non-contact tonometry. Anterior segment examination was unremarkable in both eyes.
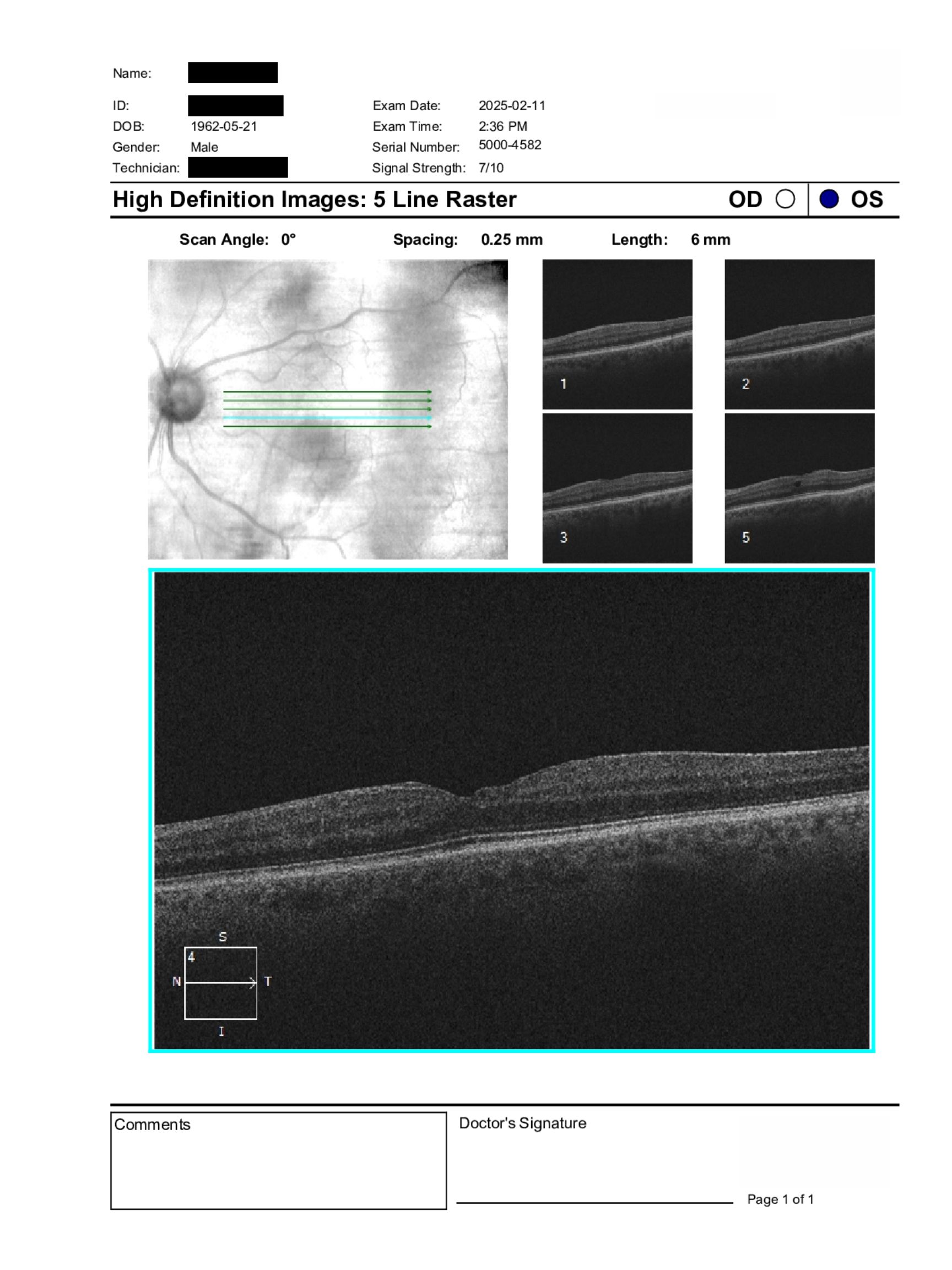
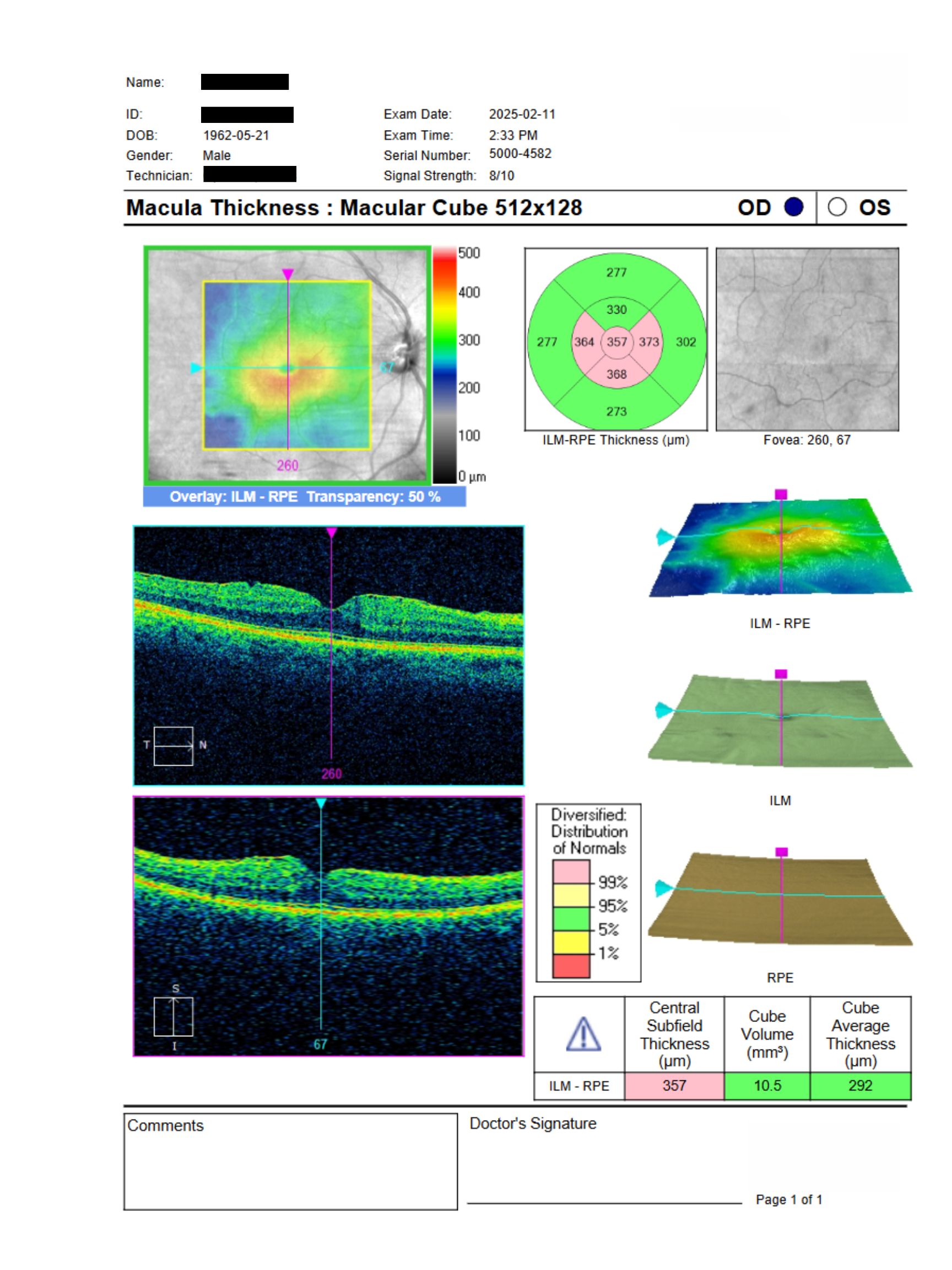
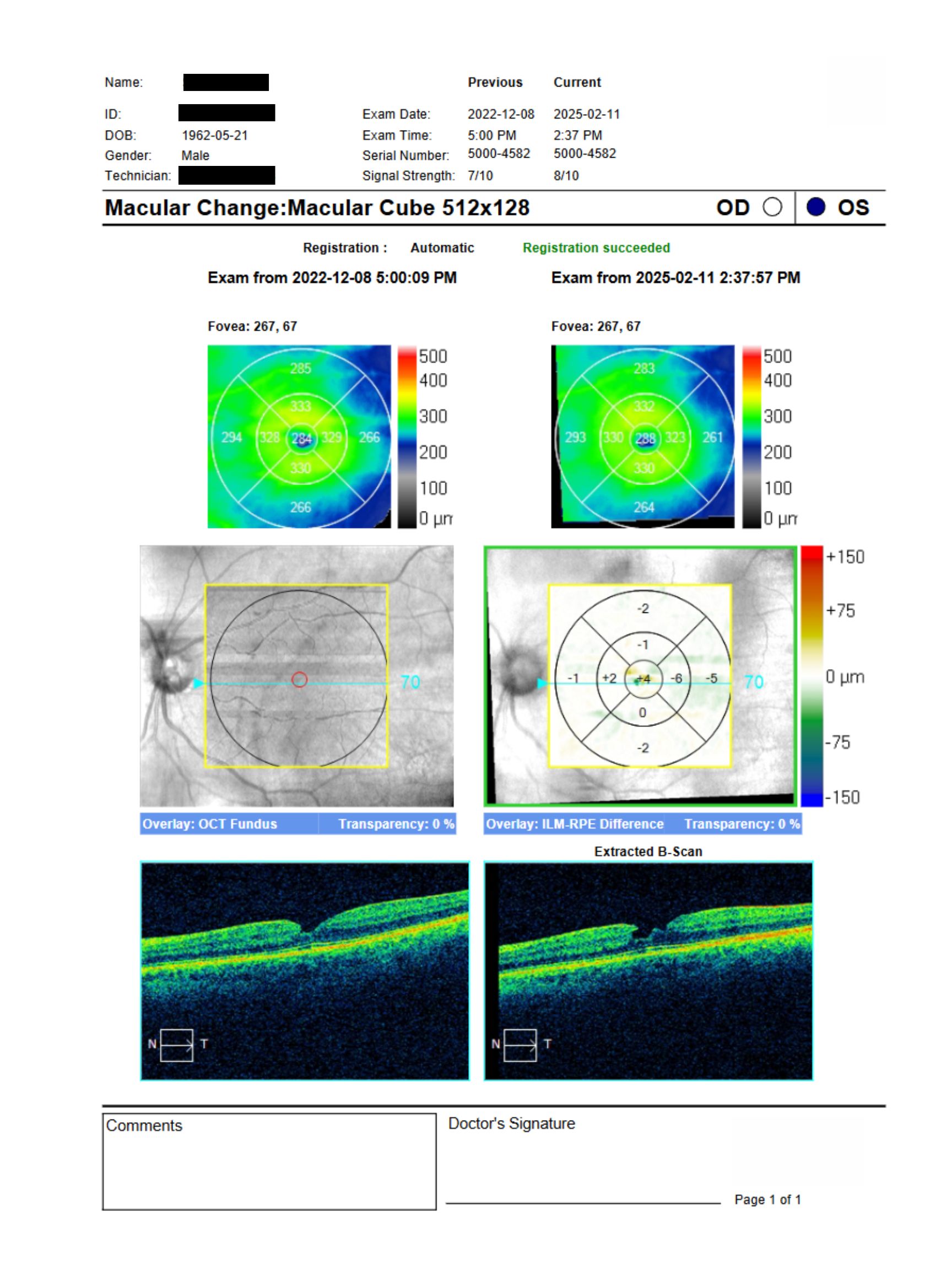
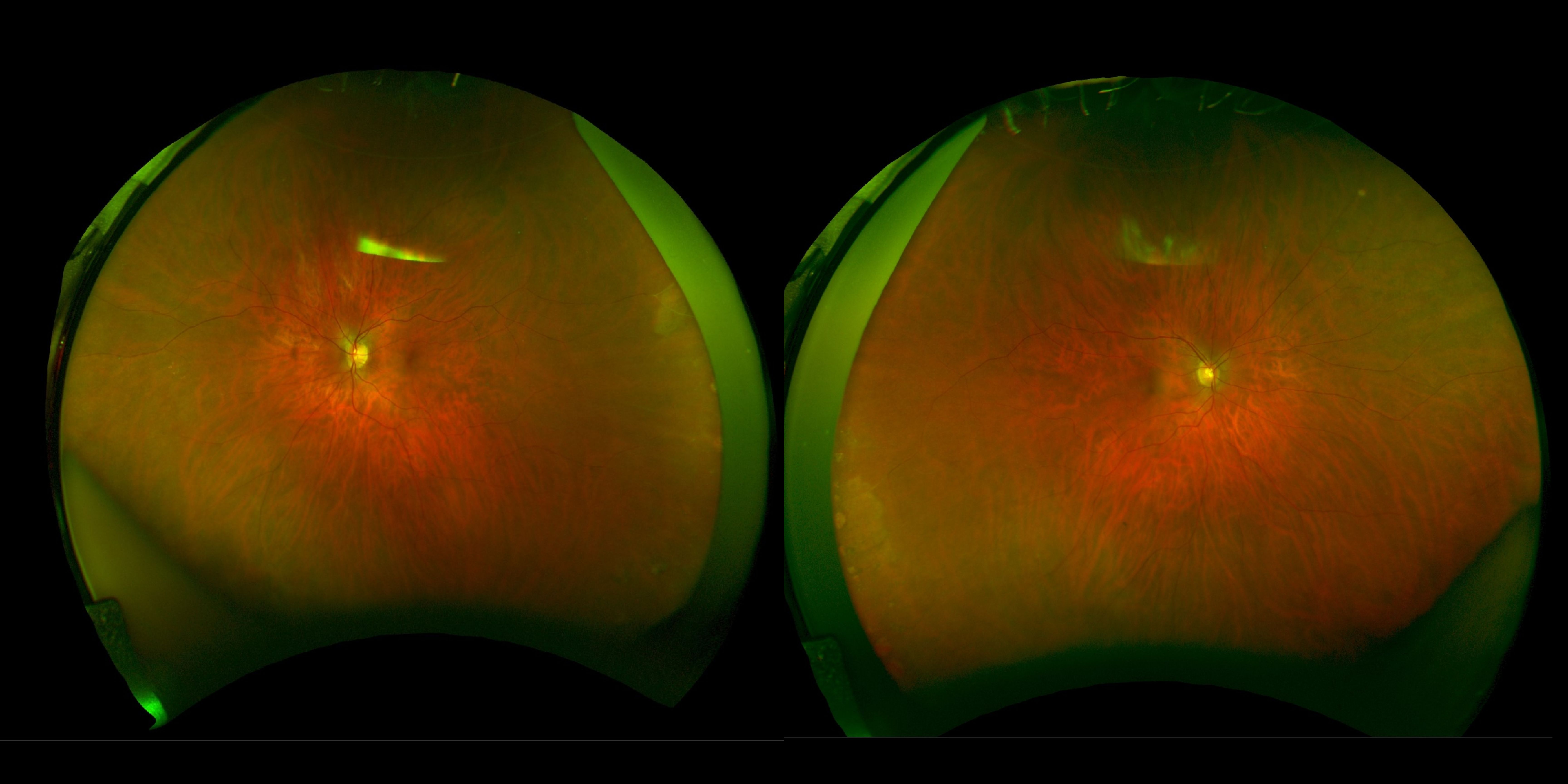
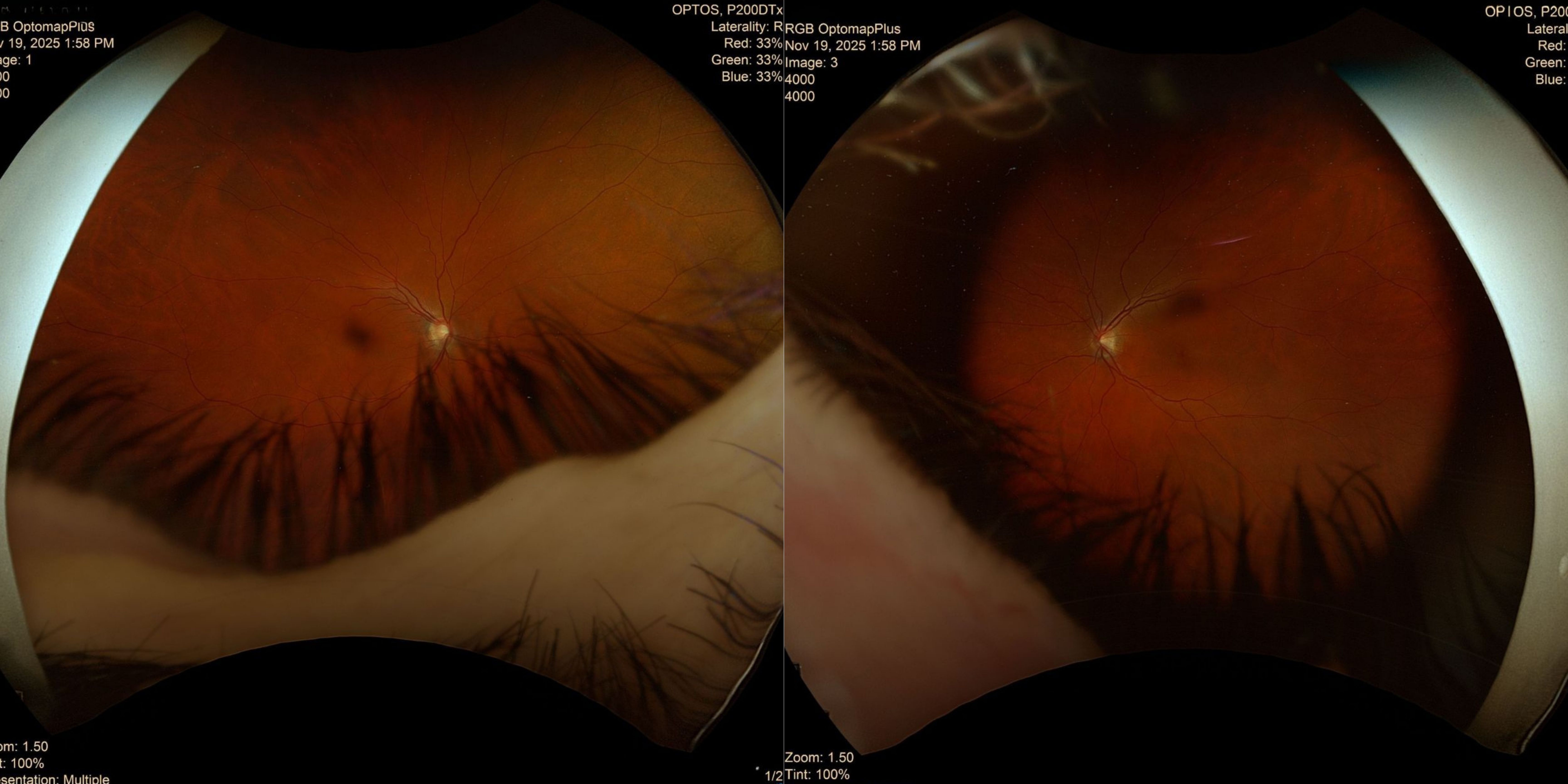
Posterior segment examination showed clear lenses and vitreous OU. Optic nerves had healthy color and clear margins with cup-to-disc ratios of 0.40 OD and 0.50 OS. Retinal vasculature was normal. Macular assessment revealed an epiretinal membrane with mild foveal distortion in the right eye and a lamellar macular hole in the left eye. The peripheral retina was clear in both eyes. OCT imaging demonstrated mild macular surface irregularity OD and a lamellar defect OS without significant interval progression.
Given the patient’s stable visual acuity and mild structural changes, would continued observation be appropriate, or should referral for surgical consideration be pursued at this stage?
An ophthalmology subspecialist provided a virtual consult within 1–2 weeks through Care1. Scroll down to see their diagnosis.
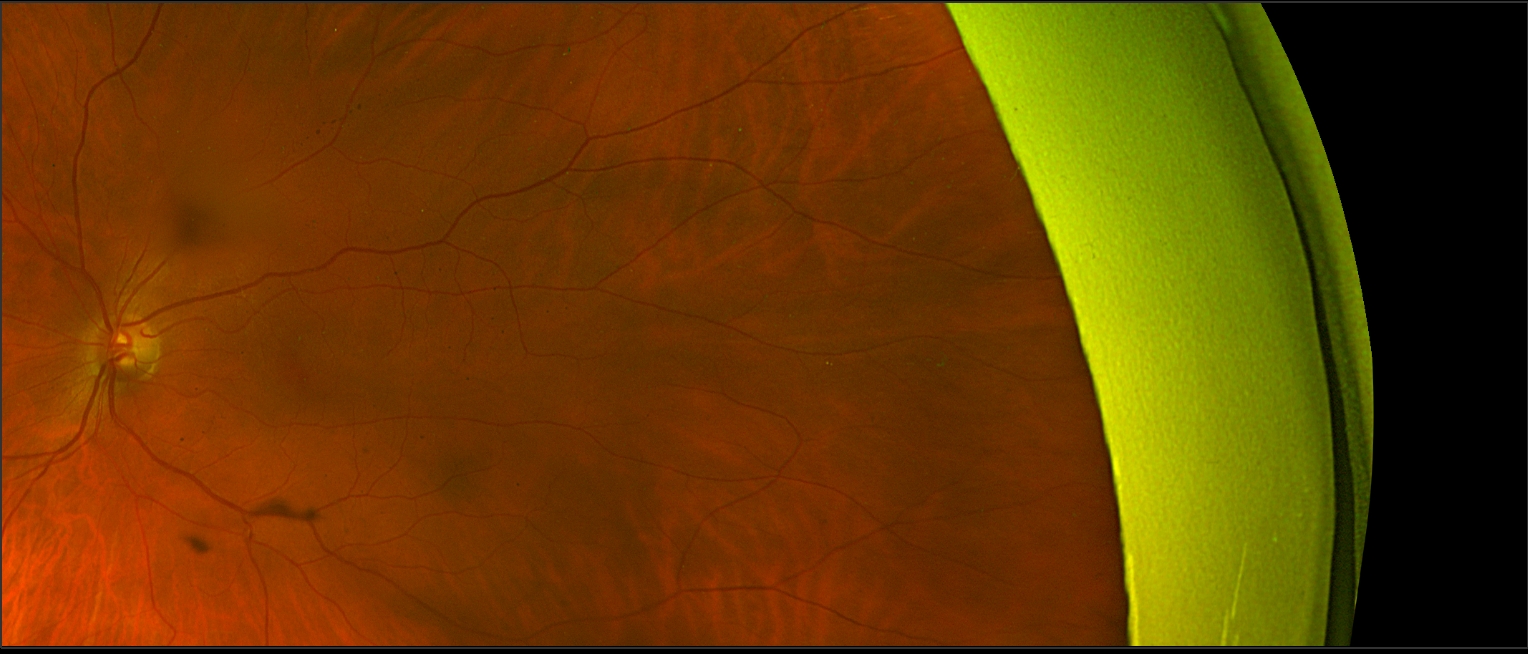
Left Fundus
Left Fundus
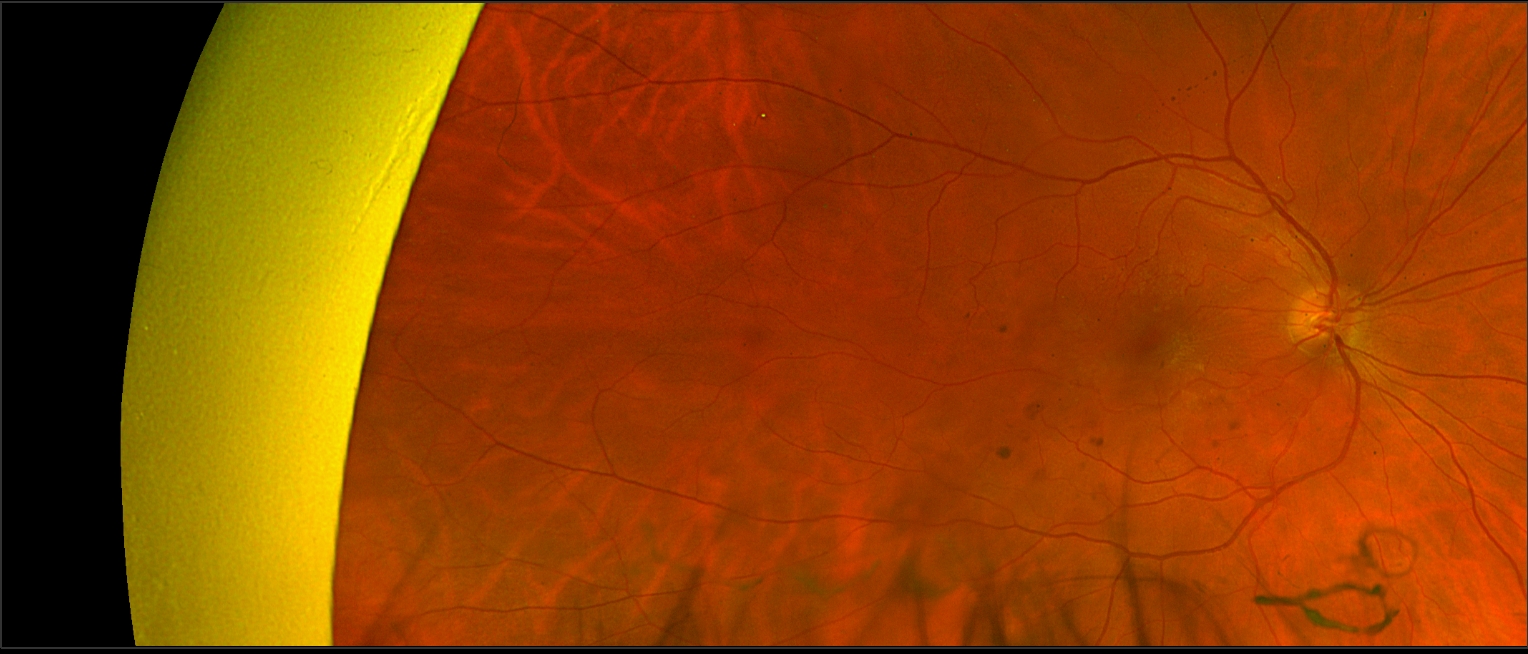
Right Fundus
Right Fundus
Care1 Subspecialist’s Key Takeaways
Since the patient maintains good vision on Snellen acuity testing and is not functionally limited, reassurance is appropriate. An epiretinal membrane with mild foveal distortion is a common age-related finding, and if the patient is not bothered by vision, observation is safer than proceeding with vitrectomy and membrane peeling.
Surgery is sometimes considered in patients with good visual acuity if symptoms significantly impact quality of life. However, when a patient is functioning well, these changes typically progress slowly and can be monitored.
Continue observation and follow-up as scheduled. Ongoing collaborative management through review of diagnostic testing is appropriate. A retina consultation is not required at this time, although a non-urgent referral can be arranged if the patient would like further discussion with a specialist.
Care1 AI’s Clinical Insight
Epiretinal membranes are fibrocellular proliferations on the inner retinal surface that may cause distortion of the macular contour and visual symptoms. Lamellar macular holes represent partial-thickness defects of the fovea and are often associated with tangential traction. Many cases remain stable for extended periods, and optical coherence tomography is essential for monitoring structural progression.
Did You Know?
Histopathologic studies have shown that epiretinal membranes are composed of glial cells, fibroblasts, and myofibroblasts capable of exerting tangential traction on the retinal surface.
Kampik A, Kenyon KR, Michels RG, Green WR, de la Cruz ZC. Epiretinal and vitreous membranes. Comparative study of 56 cases. Arch Ophthalmol. 1981;99(8):1445–1454.
Key Clinical Takeaway
Stable epiretinal membrane and lamellar macular hole can often be monitored when visual acuity remains good and structural changes are mild.
OCT imaging is critical for assessing interval progression and guiding management decisions.
Surgical referral is typically considered when there is declining visual acuity, symptomatic distortion, or evidence of progression.
Collaborative review with ophthalmology can support confidence in continued observation versus referral.