67-year-old female with reduced BCVA OD, mild cataract changes, and foveal irregularity; history of lupus and prior plaquenil exposure.
Case Study: Reduced Visual Acuity OD with Foveal Irregularity and Early Cataract
An optometrist uploaded this case to Care1.
67-year-old female with reduced OD vision. History: prior plaquenil use, lupus, anemia, AFib, arthritis. Medications: Ezetimibe, Prednisone, Apixaban, Metoprolol.
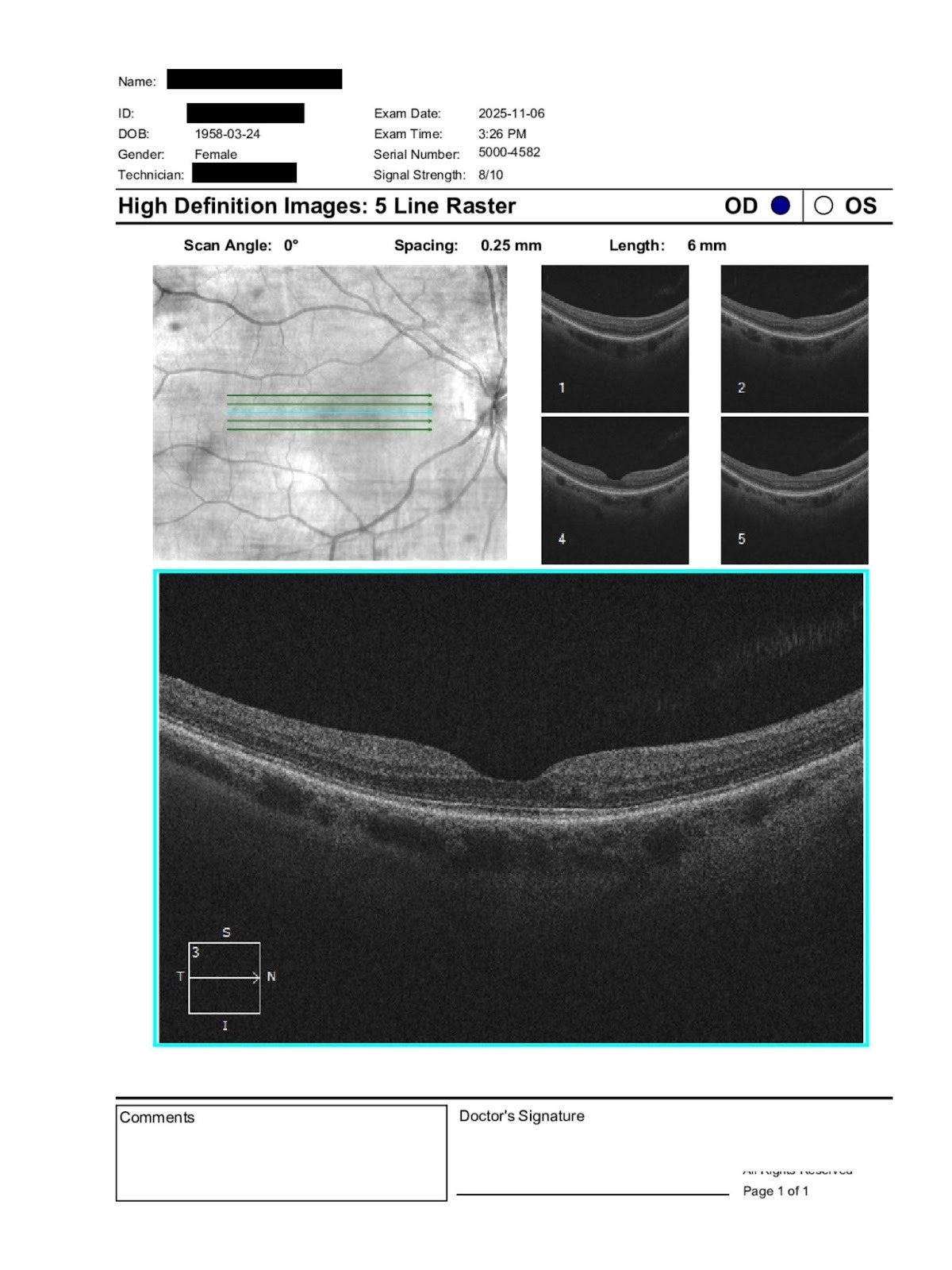
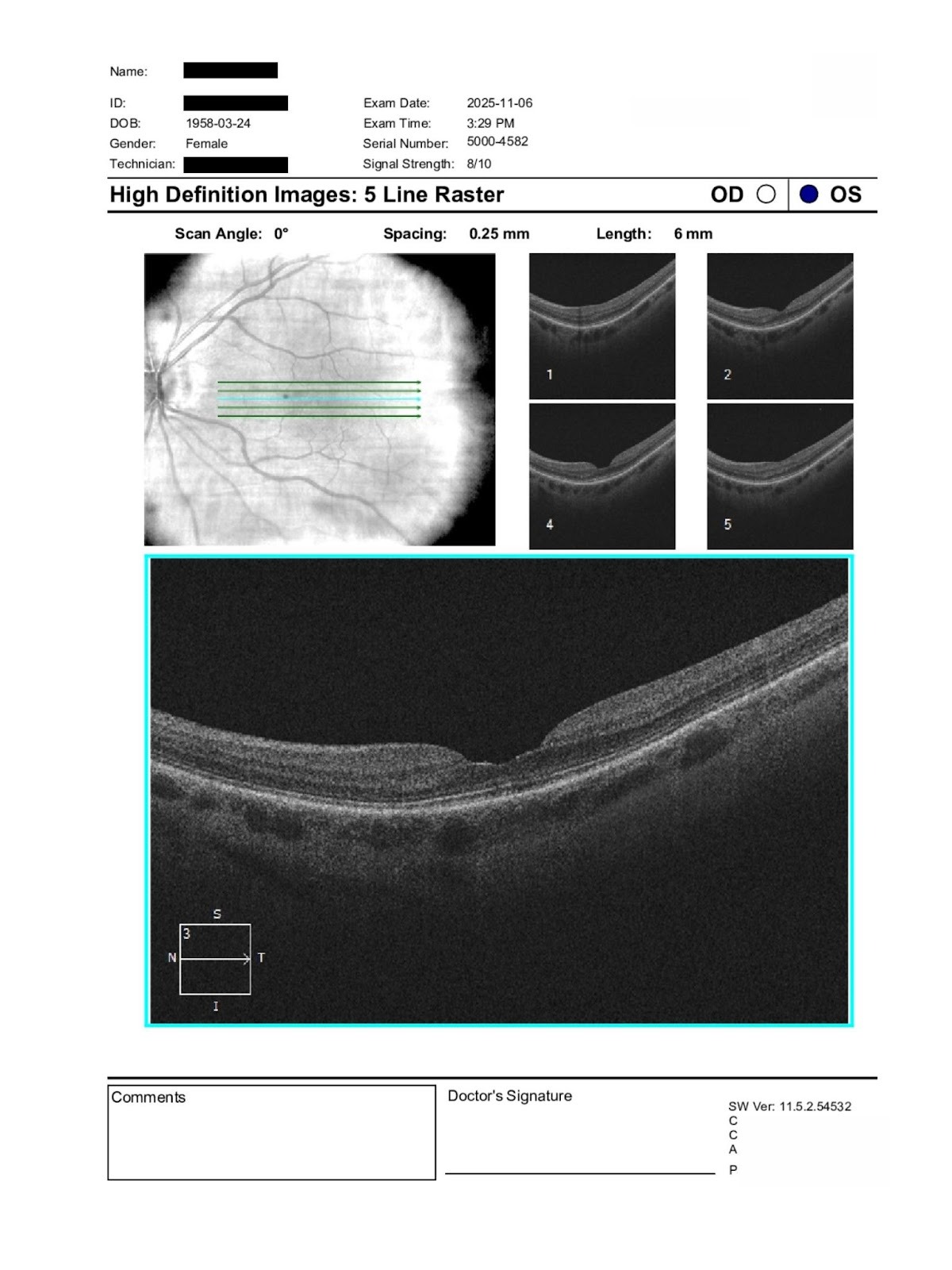
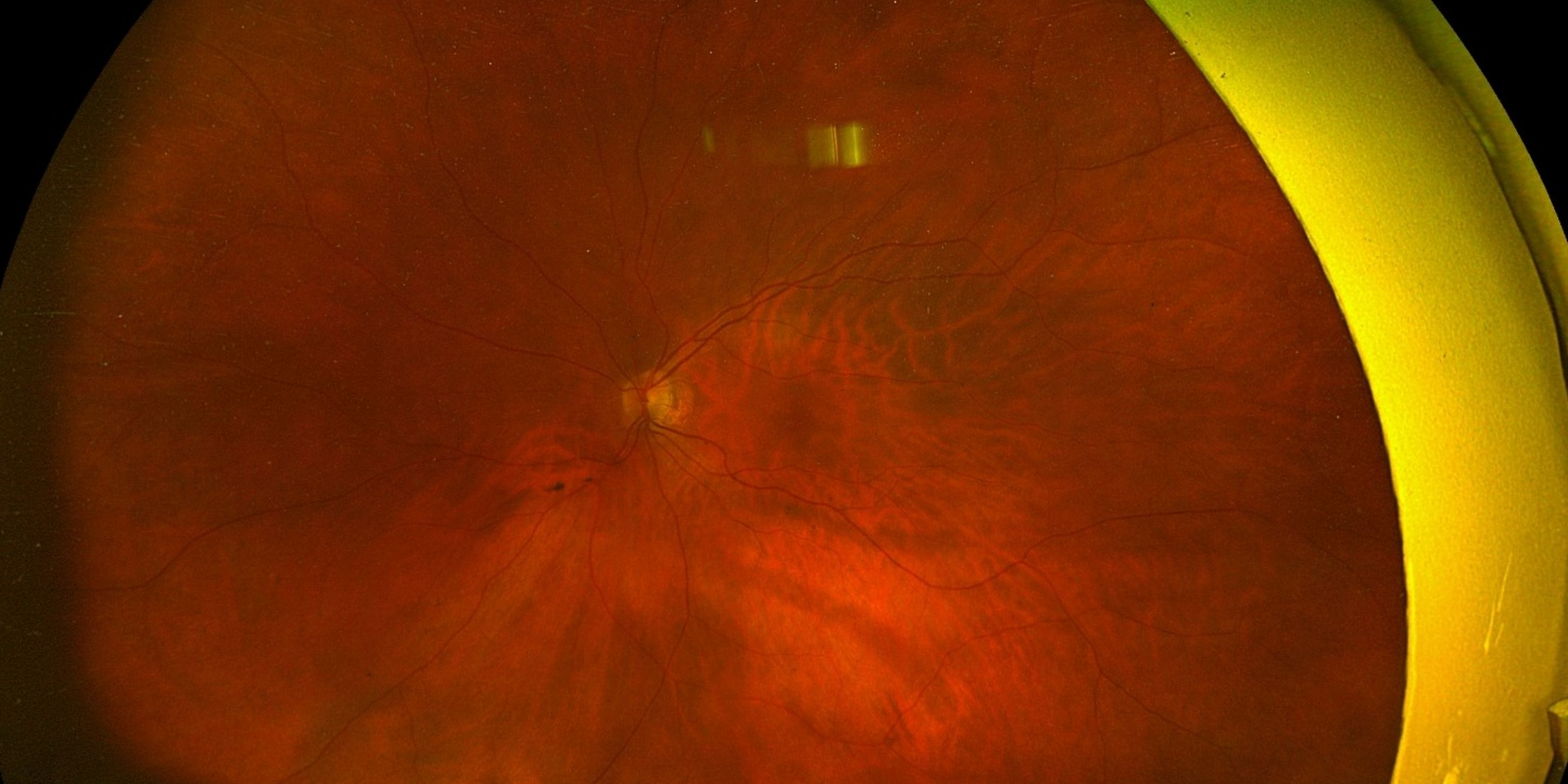
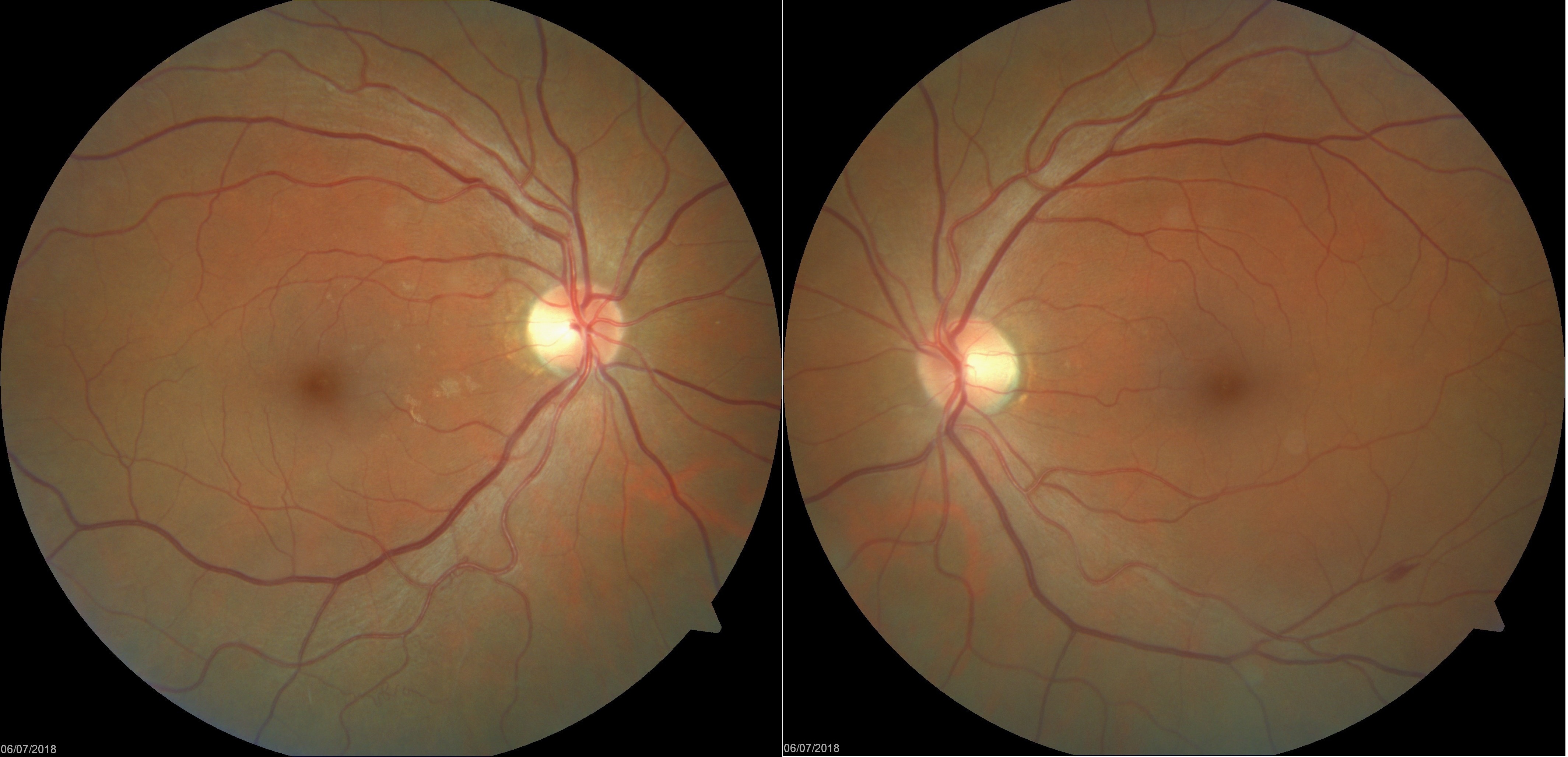
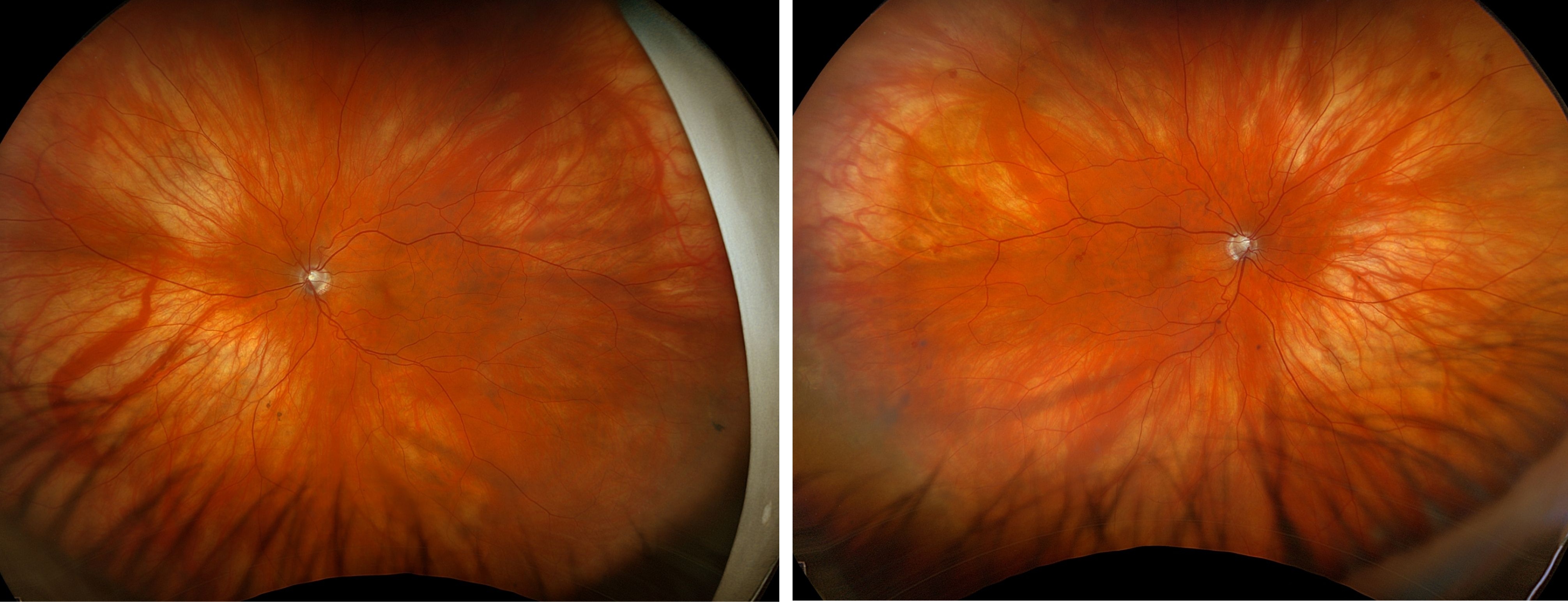
VA: 20/50 OD → 20/40 OD with refraction; 20/40 OS → 20/25– OS. IOP: 18 OD / 15 OS. Exam: mild nuclear sclerosis OU, central posterior opacity OD, tear breakup 3 sec OU (dry eye, CPAP use). Posterior: healthy discs, OD macula foveal irregularity, OS macula flat; periphery clear.
Question: With mild cataract and OD macular changes, what is the relative lenticular vs macular contribution, and is further retinal imaging/referral warranted?
A retina specialist provided a virtual consult within 1-2 weeks through Care1. Scroll below to see their diagnosis.
Care1 Subspecialist’s Key Takeaways
The reduced best corrected acuity in the right eye appears multifactorial. A small central posterior lens opacity may contribute to decreased contrast and acuity, particularly under mesopic conditions. However, the documented foveal irregularity raises concern for subtle macular structural change.
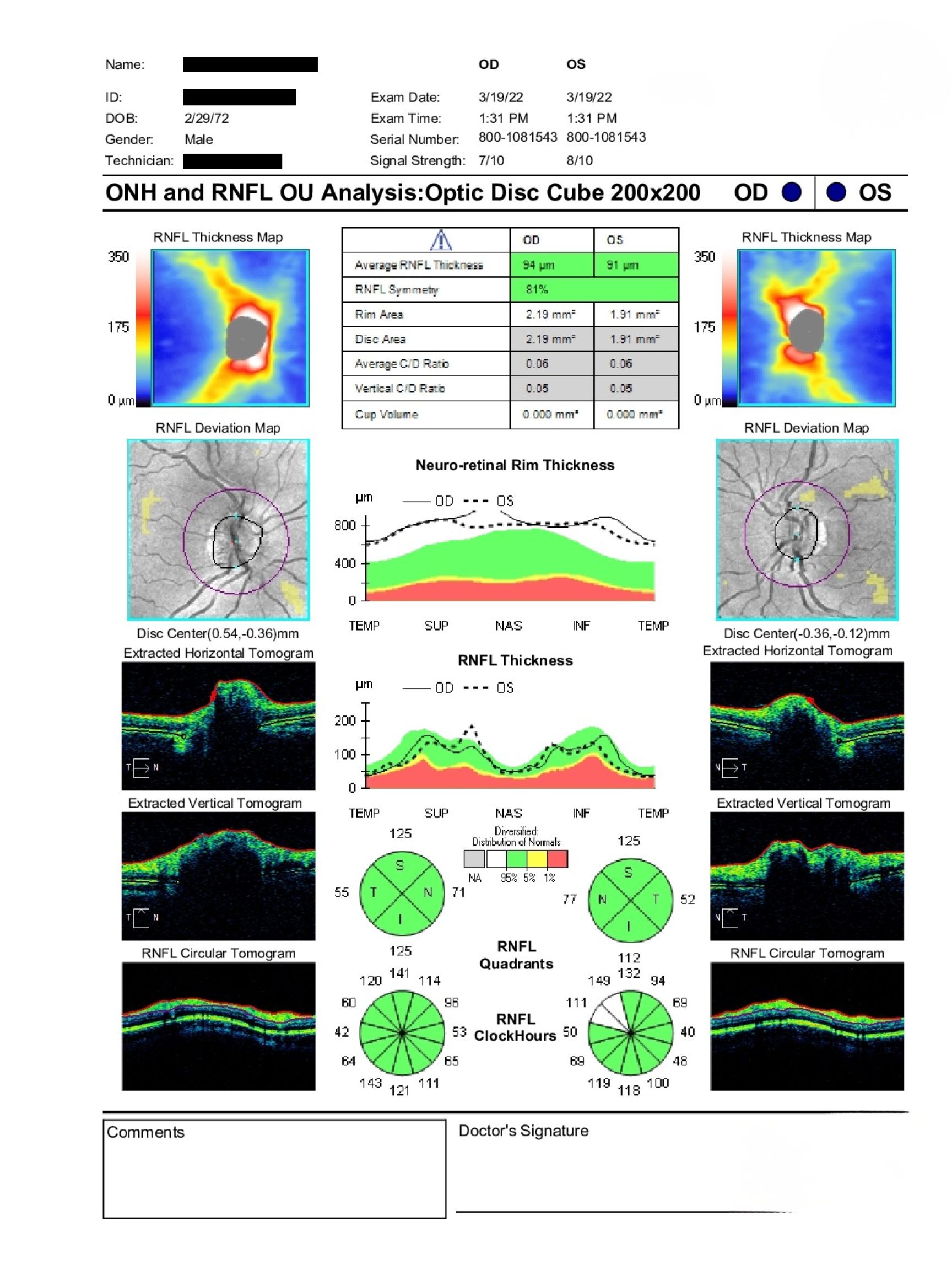
Given the history of prior hydroxychloroquine use and autoimmune disease, careful OCT review of the ellipsoid zone and parafoveal outer retina is recommended to rule out early or residual toxic maculopathy.
Dry eye disease may contribute to fluctuating blur but is unlikely to account for a stable 20 over 40 best corrected acuity in isolation.
If OCT demonstrates disruption of outer retinal layers or progressive change, in person retinal evaluation is appropriate. If imaging is stable and lens opacity correlates with symptoms, cataract progression may be the primary contributor. Close follow up is advised to monitor for progression.
Care1 AI’s Clinical Insight
When reduced acuity does not fully correlate with refractive error or lens findings, subtle macular pathology should be suspected. Foveal contour irregularities may reflect prior inflammatory, toxic, or degenerative changes and can limit visual potential even in the absence of obvious edema or hemorrhage. Optical coherence tomography is essential in distinguishing photoreceptor layer disruption from surface or lenticular causes of blur.
Did You Know?
Hydroxychloroquine retinal toxicity preferentially affects the parafoveal photoreceptors in early stages and may remain detectable on OCT even after medication cessation. Structural changes in the ellipsoid zone often precede visible fundus findings or marked visual acuity decline.
Marmor MF et al. Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy. Ophthalmology. 2016;123(6):1386–1394.
Key Clinical Takeaway
Unilateral reduction in best corrected visual acuity warrants careful macular evaluation, even when only mild cataract changes are present.
A central posterior lens opacity may contribute to reduced contrast sensitivity, but persistent acuity asymmetry should prompt assessment for subtle foveal structural abnormalities.
In patients with autoimmune disease and prior hydroxychloroquine exposure, OCT imaging is critical to evaluate outer retinal integrity, even years after medication cessation.
Ocular surface disease can amplify subjective blur but rarely accounts for stable reduced BCVA in isolation.
Collaborative evaluation between optometry and ophthalmology helps distinguish refractive, lenticular, surface, and retinal contributors to visual decline while guiding appropriate monitoring or referral.

.jpg)