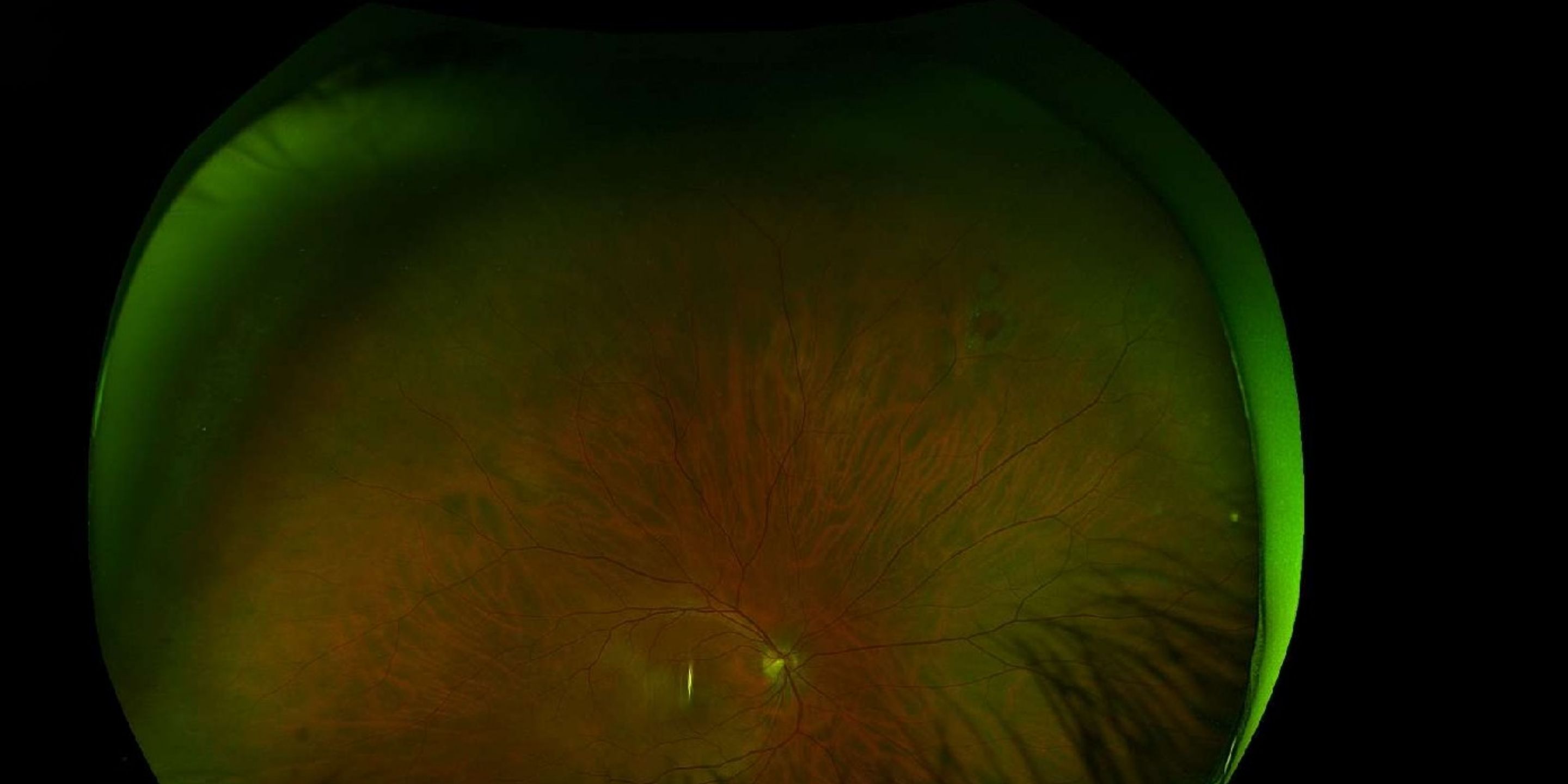
48-year-old male with asymptomatic longstanding superonasal operculated retinal hole OD, slightly larger than prior exam; question of prophylactic laser retinopexy.
Case Study: Longstanding Operculated Retinal Hole – Observe or Laser?
An optometrist uploaded this case to Care1.
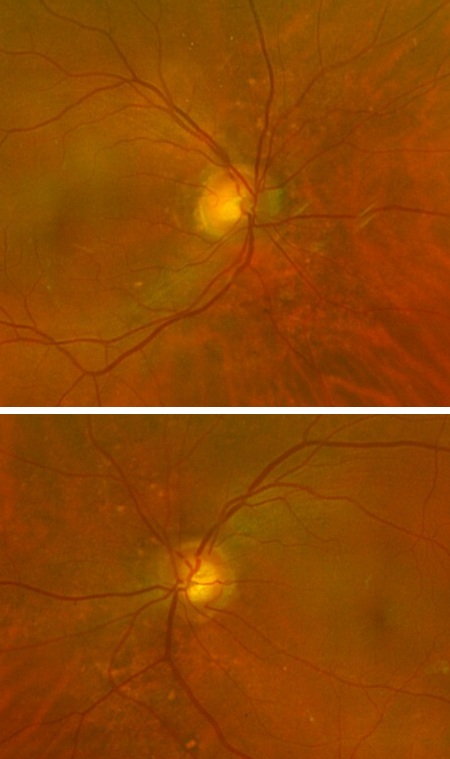
A 48-year-old male presented for evaluation of a known right retinal hole and is asymptomatic. Ocular history includes a childhood baseball injury OD and LASIK in 2013 (−2.50 OU pre-op). Unaided VA was 20/20 OD and 20/25 OS (pinhole 20/20 OS). IOP was 14 mmHg OU. Posterior segment exam showed healthy optic nerves (CDR 0.3 OU) and normal maculae.
Peripheral exam revealed a superonasal operculated retinal hole OD, slightly larger than in 2023, without tobacco dust, hemorrhage, tear, detachment, or subretinal fluid. Is prophylactic laser retinopexy indicated or is observation appropriate?
A retina specialist provided a virtual consult within 1-2 weeks through Care1. Scroll below to see their diagnosis.
Care1 Subspecialist’s Key Takeaways
This appears to be a longstanding operculated retinal hole with no evidence of persistent vitreoretinal traction. Operculated holes generally occur after focal vitreous traction avulses a plug of retinal tissue, relieving traction and lowering the risk of progression to retinal detachment.
In the absence of subretinal fluid, lattice degeneration, vitreous hemorrhage, or tobacco dust, observation is often appropriate. Slight enlargement over time can occur and does not automatically indicate increased detachment risk if the lesion remains traction free.
Prophylactic laser retinopexy may be considered in select cases with high risk features, such as significant myopia, history of retinal detachment in the fellow eye, or symptomatic flashes and floaters. In asymptomatic patients with stable findings, careful monitoring and patient education regarding warning symptoms is reasonable.
Close follow up with repeat dilated peripheral retinal examination is recommended.
Care1 AI’s Clinical Insight
Operculated retinal holes differ from horseshoe tears in that vitreoretinal traction has typically been released at the time the operculum forms. This reduces ongoing mechanical stress at the lesion margin. The primary factors that increase detachment risk include persistent traction, associated subretinal fluid, and peripheral degenerative changes. Careful documentation of size, location, and surrounding retina allows longitudinal comparison and informed management decisions.
Did You Know?
Operculated retinal holes have a substantially lower risk of progressing to rhegmatogenous retinal detachment compared to horseshoe retinal tears because the tractional component has already separated from the retina.
Byer NE. Natural history of asymptomatic retinal breaks and lattice degeneration. Ophthalmology. 1989;96(9):1395–1401.
Key Clinical Takeaway
Operculated retinal holes are typically low risk for progression when vitreoretinal traction has been released.
Absence of subretinal fluid, lattice degeneration, or tobacco dust significantly reduces concern for imminent retinal detachment.
Slight enlargement over time does not necessarily mandate laser treatment if the lesion remains operculated and traction free.
Patient education regarding symptoms of retinal tear and detachment is critical in conservative management.
Shared decision making between optometry and ophthalmology supports individualized management based on risk factors, symptoms, and documented change.