68-year-old patient with asymmetric optic nerve cupping, borderline IOPs, thin corneas, and normal OCT/VF findings.
Case Study: Asymmetric Optic Nerve Cupping
An optometrist uploaded this case to Care1.
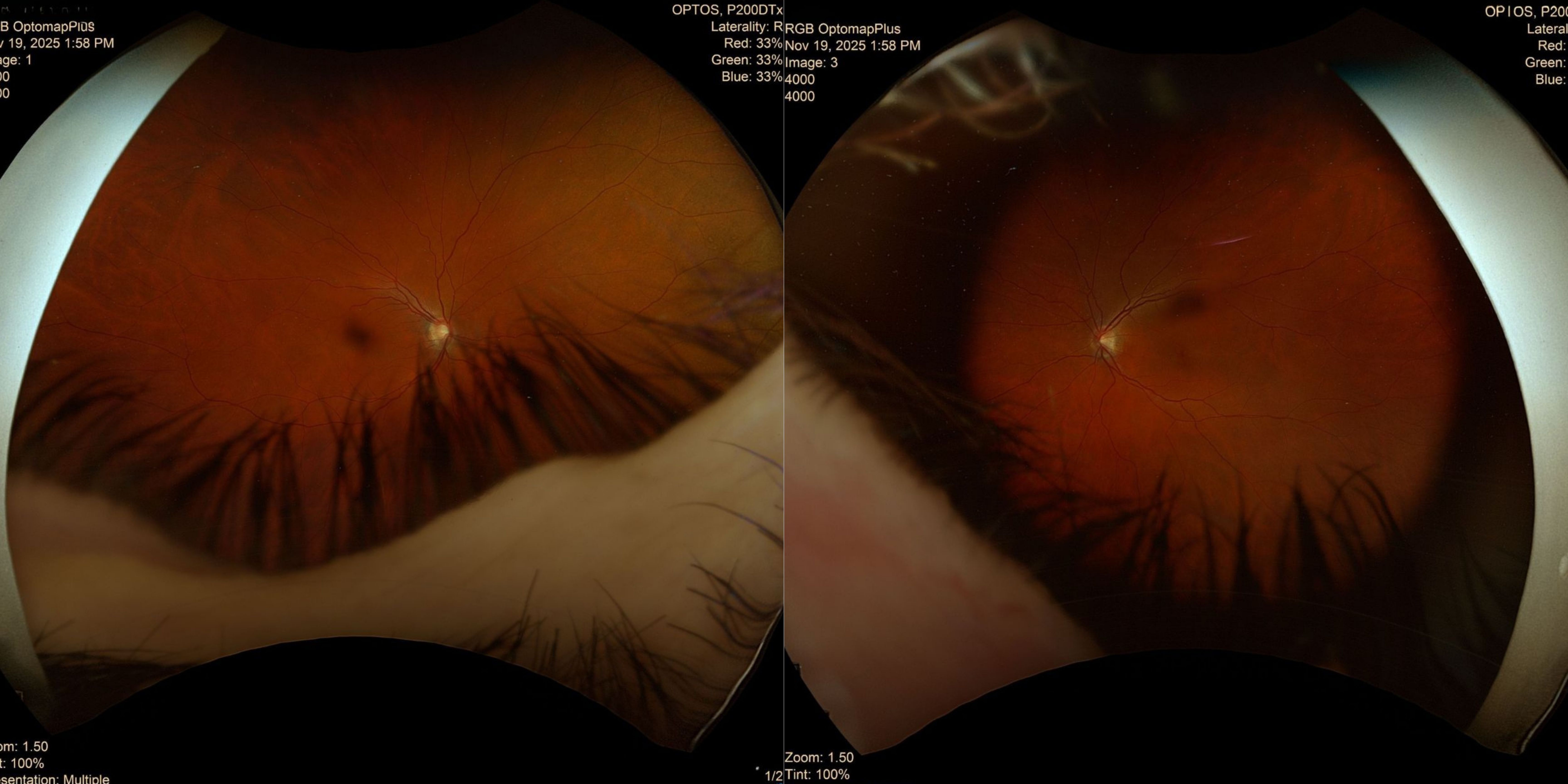
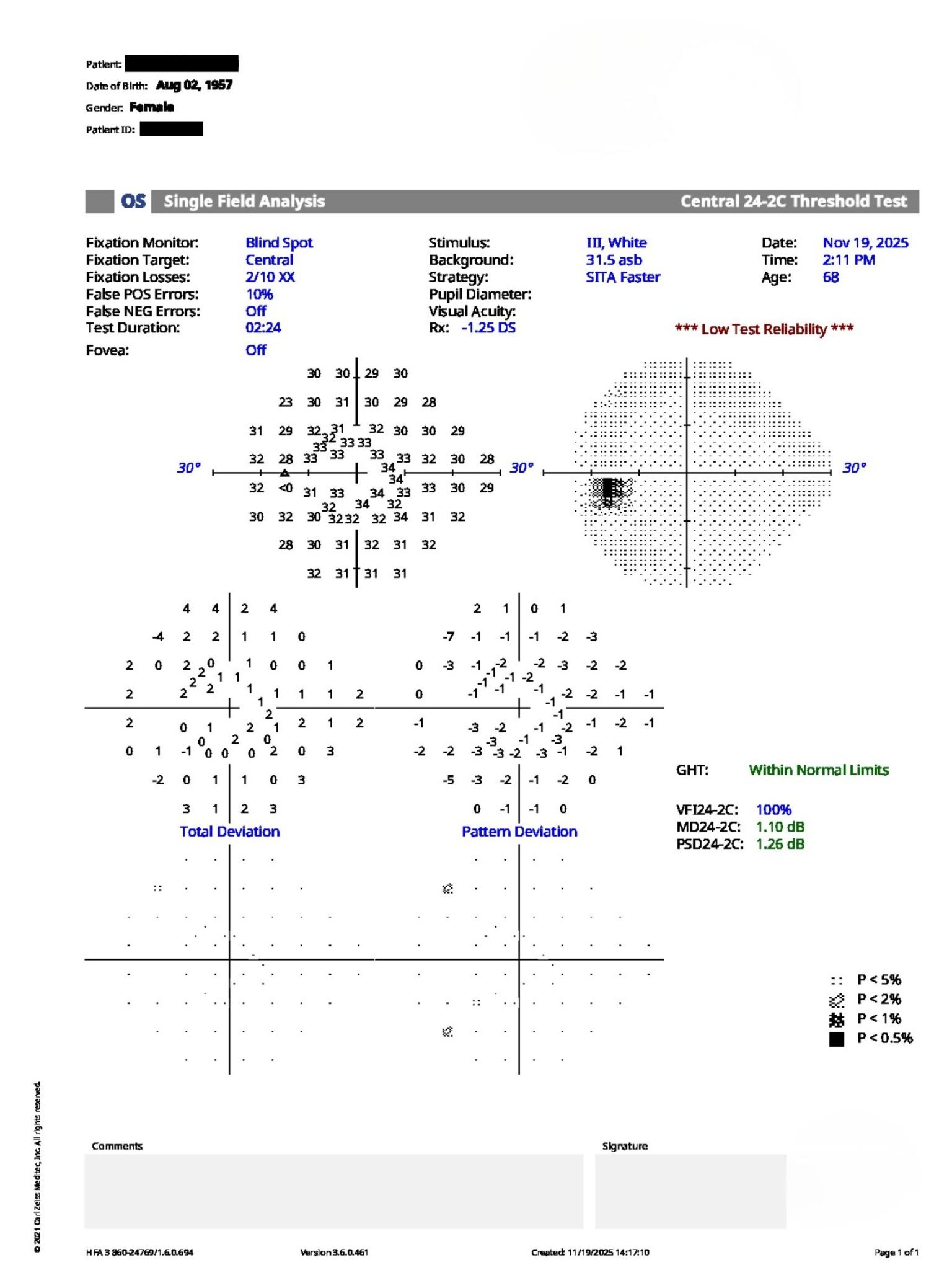
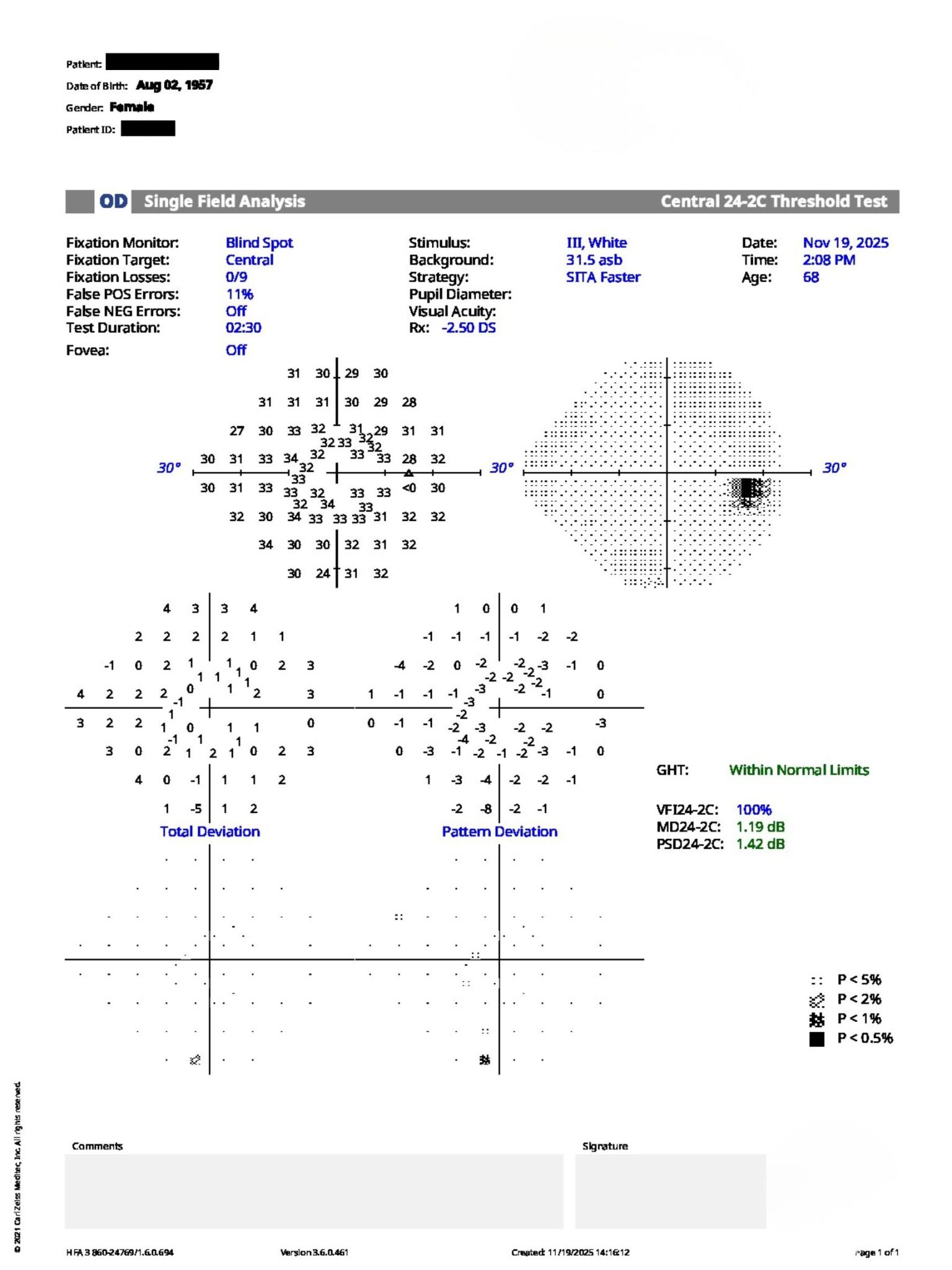
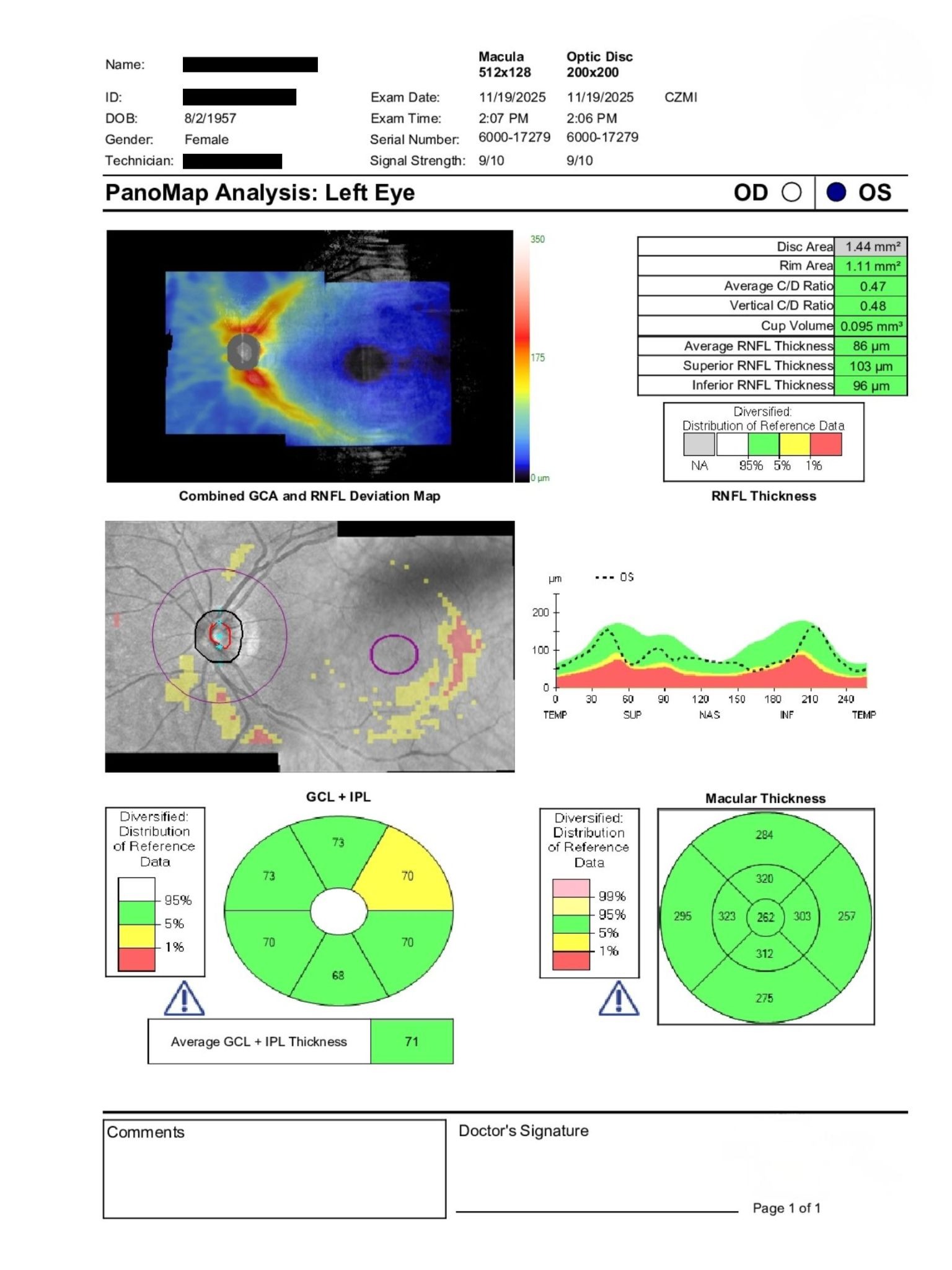
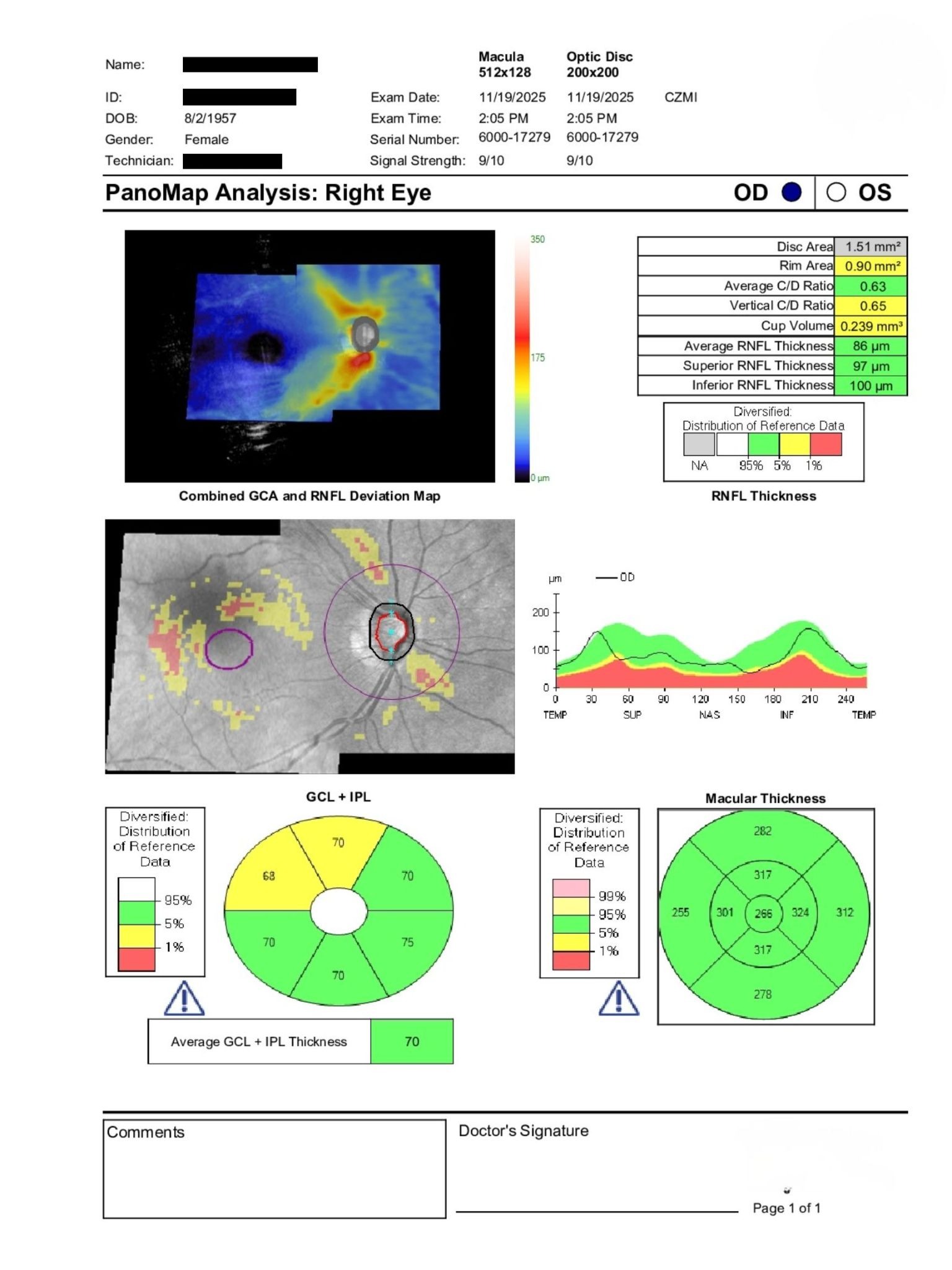
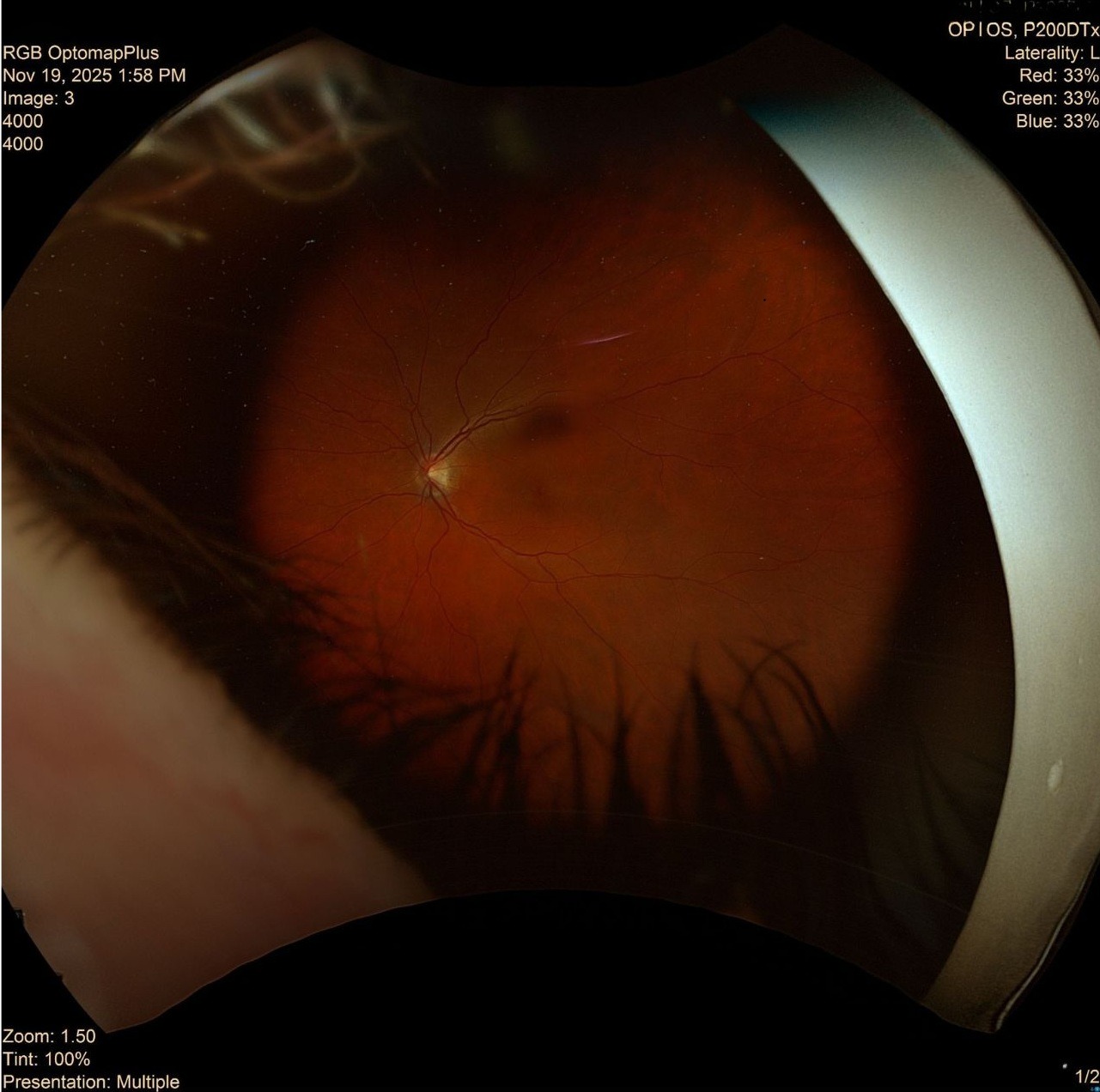
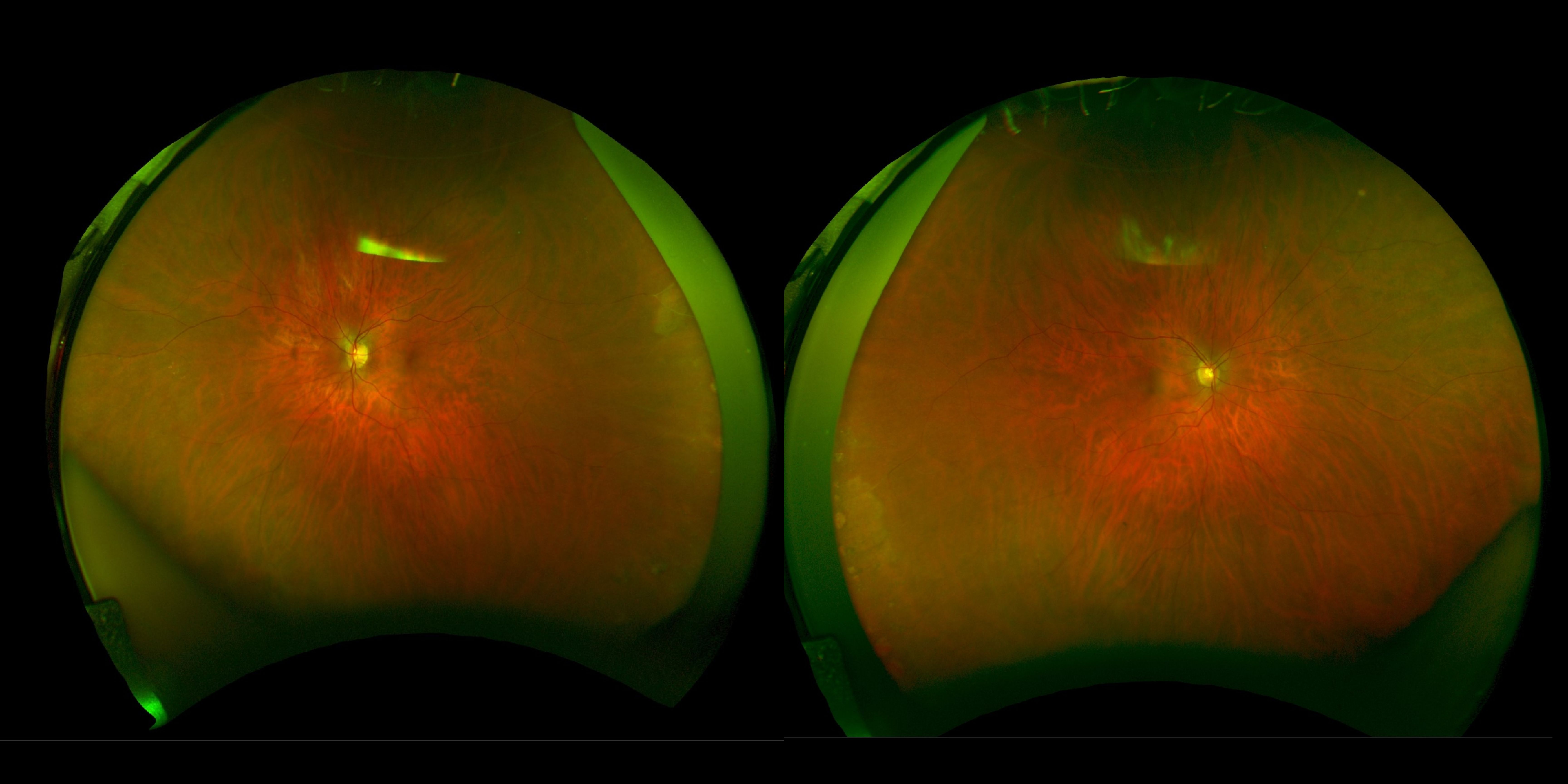
An optometrist referred a 68-year-old patient for glaucoma evaluation due to asymmetric optic nerve cupping and borderline intraocular pressures. Best corrected visual acuity was 20/25 OD and 20/20 OS. IOP measured 20 mmHg OD and 19 mmHg OS with thin corneas. Anterior segment examination showed mild blepharitis, dry eye disease, conjunctival injection, and superficial punctate keratitis. Posterior segment assessment demonstrated asymmetric optic nerve cupping (OD greater than OS), while OCT RNFL and visual field testing remained within normal limits.
Given the asymmetric optic nerve appearance, family history, thin corneas, and normal OCT/VF results, should additional investigation or closer monitoring be considered?
An ophthalmology subspecialist provided a virtual consult within 1-2 weeks through Care1. Scroll below to see their diagnosis.
Care1 Ophthalmologist's Teleconsult
The optic nerves demonstrate longstanding asymmetry, with a cup-to-disc ratio of approximately 0.60 OD and 0.30 OS. Intraocular pressures remain within the target range, and both OCT RNFL imaging and visual field testing are reassuring overall.
Risk factors include optic nerve asymmetry, family history, myopia, thin corneas, and borderline structural findings. However, stable visual fields, largely normal OCT findings, and the absence of definitive progression support continued surveillance.
Regular follow-up with OCT RNFL imaging, visual field testing, and IOP monitoring remains appropriate to assess for any future structural or functional change.
Care1 AI's Clinical Insight
Asymmetric Optic Nerve Cupping
Asymmetric optic nerve cupping is an important clinical finding during glaucoma assessment. Evaluation includes comparing optic nerve appearance between eyes, correlating structural findings with OCT RNFL imaging, and assessing for corresponding visual field abnormalities. Large physiologic cups, myopia, optic disc size variation, and glaucomatous optic neuropathy can all contribute to asymmetry. Structural optic nerve changes may precede detectable visual field defects, making longitudinal monitoring essential.
Practice at the highest level of medicine
✔ Specialist consults within 1-2 weeks ✔ AI-powered clinical support ✔ Greater confidence in complex decision making
A classic AAO reference notes that a cup-to-disc ratio asymmetry greater than 0.2 occurs in fewer than 1% of individuals without glaucoma, making significant asymmetry an important finding during optic nerve evaluation. This highlights why careful assessment of disc size, RNFL structure, and visual field correlation is essential when asymmetry is present.
Reference: American Academy of Ophthalmology. BCSC Section 10: Glaucoma. San Francisco, CA: American Academy of Ophthalmology; 2019-2020.