.avif)
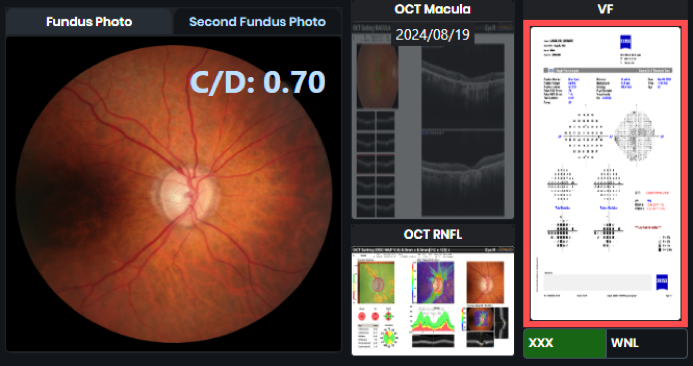
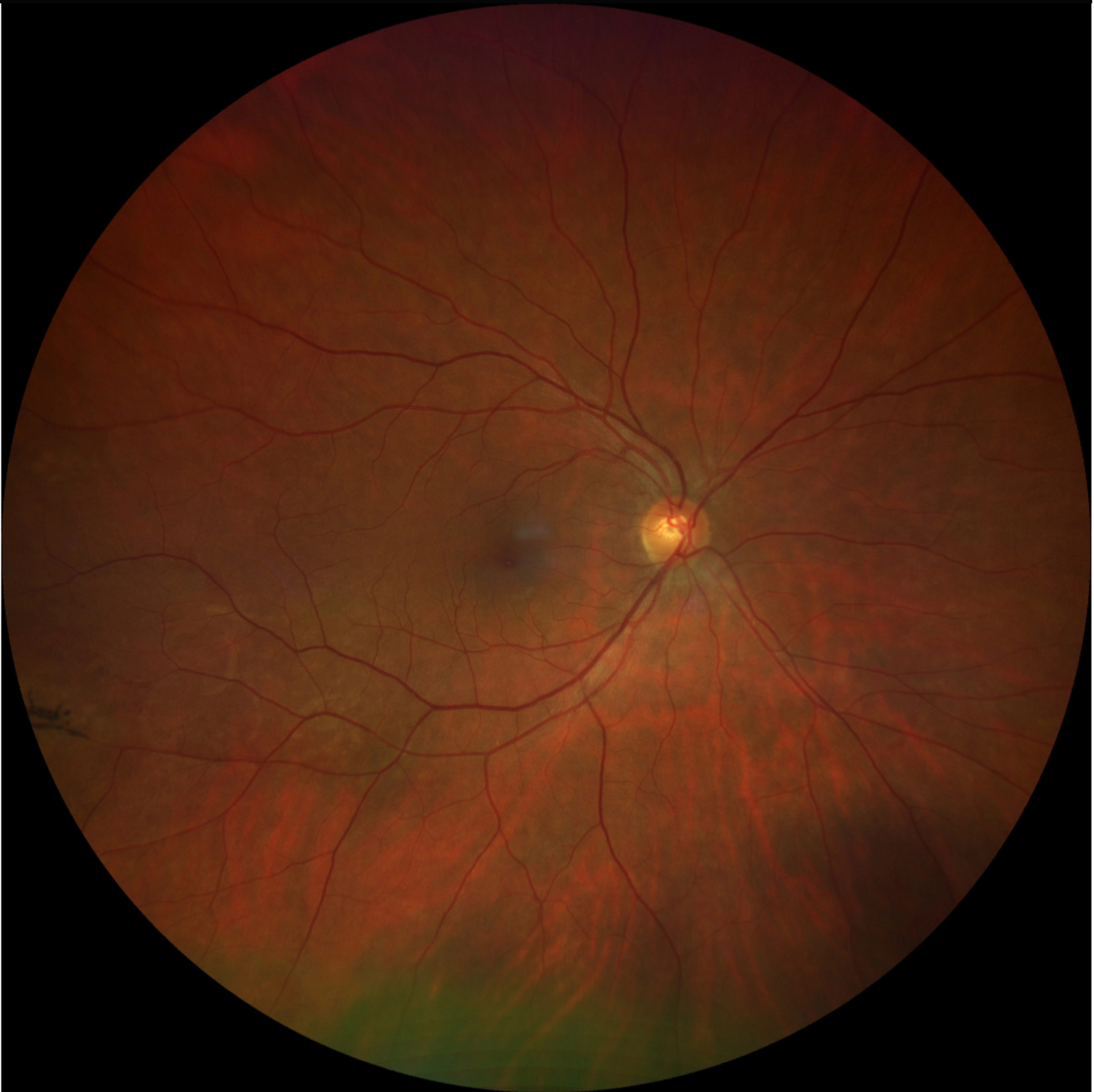
An 80-year-old male presents for follow-up on bilateral macular edema. Initially responsive to Nevanac, the edema has now worsened despite stable BCVA at 20/30 OU.
A retina specialist provided a virtual consult within 1-2 weeks through Care1. Scroll below to see their diagnosis.
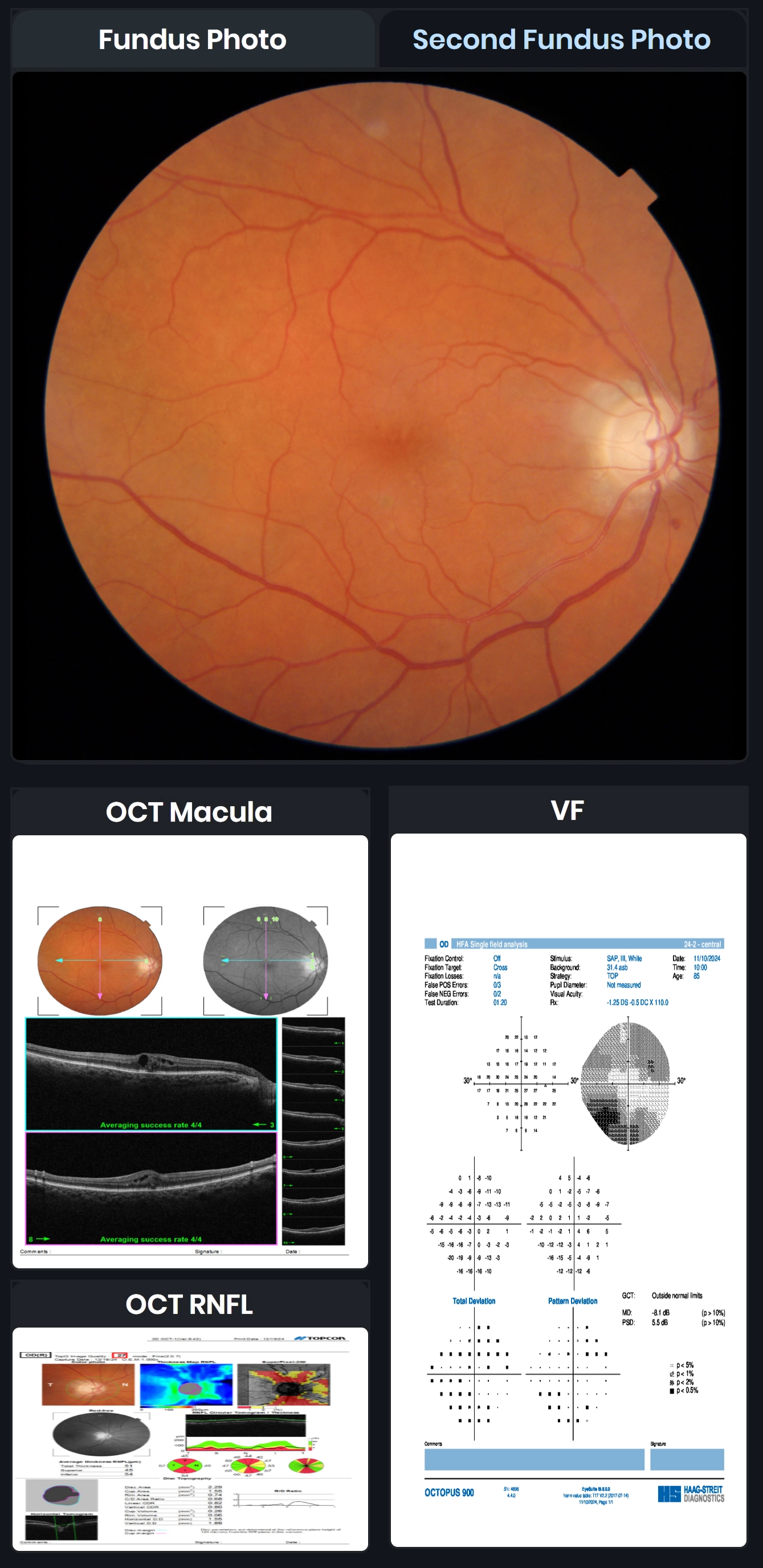
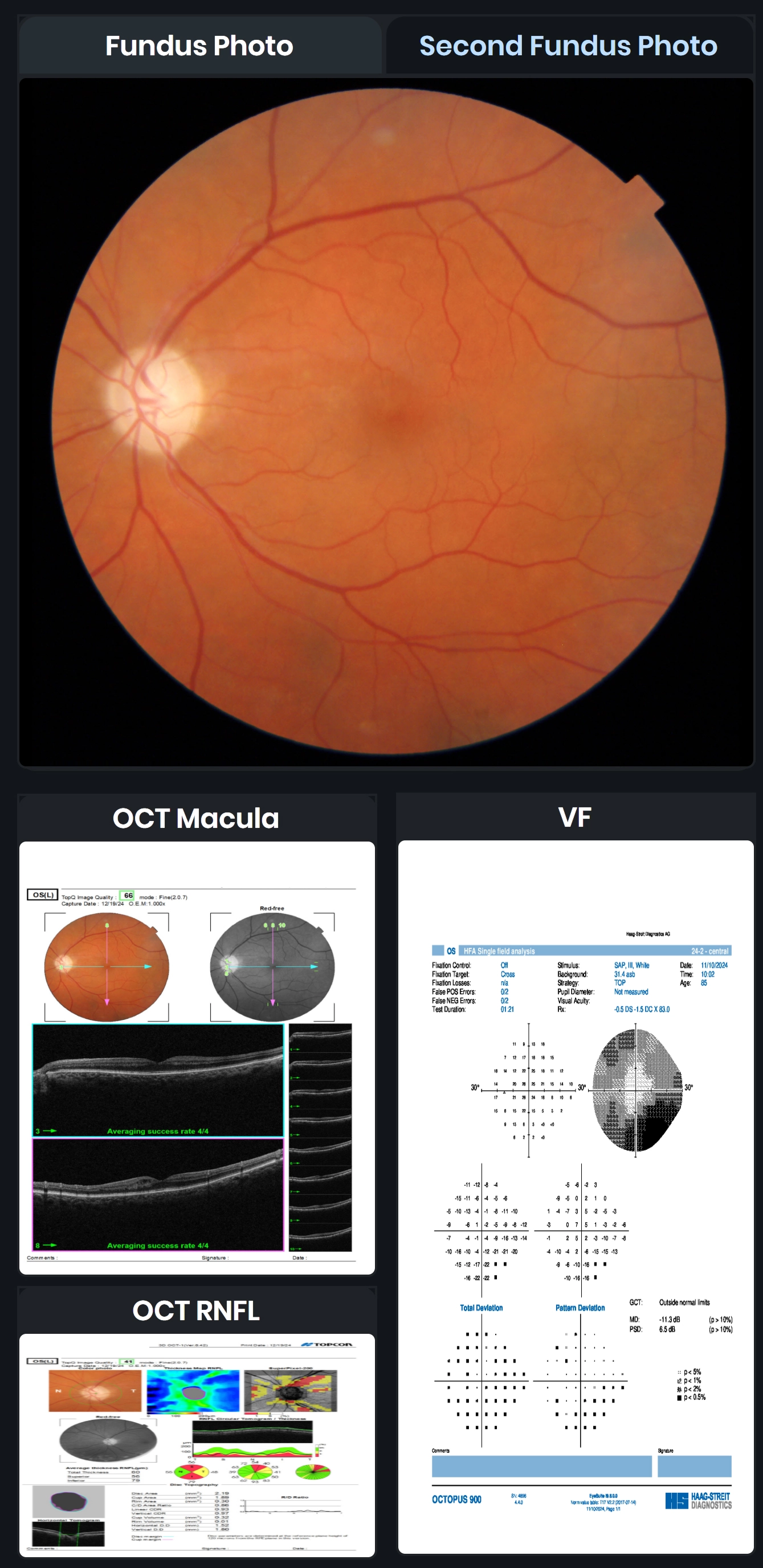
Cystoid Macular Edema (CME) is a leading cause of central vision loss, resulting from fluid accumulation in the retina due to blood-retinal barrier disruption. It commonly appears in conditions like diabetic macular edema, vein occlusions, post-cataract surgery (Irvine-Gass), and uveitis. OCT and FA imaging are crucial for diagnosis, revealing characteristic cystic spaces and petaloid leakage patterns. While many cases resolve within months, persistent CME may require NSAIDs, corticosteroids, CAIs, anti-VEGF therapy, or even vitrectomy for tractional cases. Recent research also challenges the long-standing myth that prostaglandin analogs significantly increase CME risk in glaucoma patients.
✔ Deliver the highest standards of care
✔ Increase patient satisfaction and retain patients
✔ Stimulate revenue
Recent research challenges the long-standing myth that prostaglandin analogs significantly increase CME risk in glaucoma patients.(Niyadurupola N, Brodie J, Patel T, et al. Topical prostaglandin analogue use and cystoid macular oedema following uneventful cataract surgery: a randomised control trial. Br J Ophthalmol. 2022;106(12):1662-1666. doi:10.1136/bjophthalmol-2021-319149)